Standards for evaluating clinical
Methods for such trials have been established and tested in a variety of clinical settings, usually under everyday conditions. 70, 109, 162 They are particularly valuable when physicians or patients are uncertain about the efficacy of treatment for symptomatic diseases. Controls can be incorporated even in this kind of trial. Such trials can be double-blinded and can involve cross-over designs in which the patient is treated with alternating treatments, such as placebo-drug-placebo, or one drug followed by another drug Most importantly, as with any other clinical trial, a single patient trial should be designed to permit objective comparison between treatments.
Analgesia
· There are medical conditions or patients in which they are more effective than any currently available medication.
· They have a broad clinical spectrum of efficacy and a unique side effect profile that differs from other analgesics.
· They have synergistic interactions with other analgesics.
· They exhibit "side effects" which are considered useful in certain clinical situations.
· Their efficacy is enhanced in patients who have developed tolerance to opioids.
partially overlap with those activated by opioids but through pharmacologically distinct mechanisms (see chapter 2). This means that they would likely have a different side effect profile and perhaps additive or synergistic analgesic efficacy.
Clinical studies with cannabinoids
Experimentally-induced acute pain
Cancer Pain
Surgical Pain
anesthetic agent within 24 hours of the test drug were excluded from the study. On average, pain relief was significantly greater for the levonantradol-treated patients than for the placebo-treated patients. Because the authors do not report the number or the percent of people who responded, it is not clear whether this average represents consistent pain relief for all levonantradol-treated patients or whether some people experienced great relief and a few experienced none.
Case reports and surveys
Migraine Headaches
anatomical correlate between cannabinoid effects on the brain and their possible role in migraine relief:
Conclusions and Recommendations
Basic Pain Research
Clinical Pain Research
· Patients on chemotherapy, especially for the treatment of mucositis, nausea and anorexia
· Postoperative pain patients as an opioid adjunct to determine whether nausea and vomiting from opioids are reduced.
· Patients with spinal cord injury, peripheral neuropathic pain, or central post-stroke pain.
· Patients with chronic pain and insomnia.
· AIDS patients with cachexia, AIDS neuropathy, or any significant pain problem.
combinations. As with any clinical study on analgesic drugs, it will be important to investigate the development of tolerance and physical dependence. These are not, of themselves, reasons to preclude the use of cannabinoids as analgesics, but such information is essential to the management of many drugs to which patients develop tolerance or physical dependence.
Nausea and Vomiting
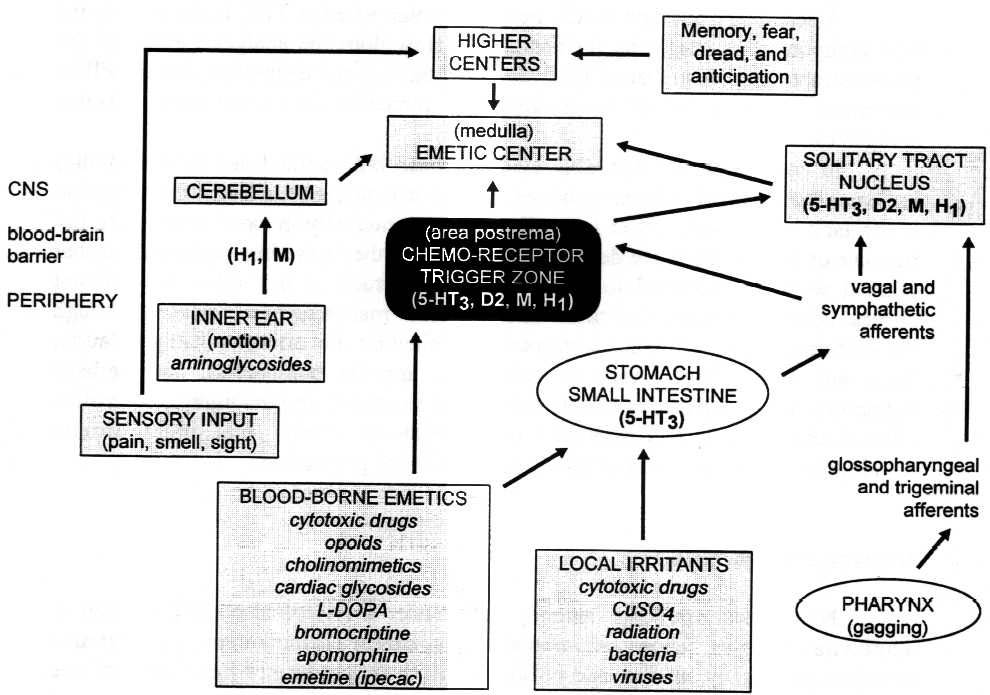
FIGURE 4.1 Emesis-stimulating pathways
Chemotherapy-Induced Nausea and Vomiting
a The visual analog scale is a continuous line representing all possible levels of a particular sensation. It is an estimation of a patient's subjective evaluation and not a true measurement. Patients select a point anywhere on the line to demonstrate the level of sensation they are experiencing, with one end representing one extreme, such as no sensations and the other end representing the opposite extreme, such as a maximum level of that sensation.
THC/Marijuana Therapy for Chemotherapy-Induced Nausea and Vomiting
Antiemetic Properties of THC
psychoactive than THC 153, but was found to completely
block both acute and delayed chemotherapy-induced emesis in a
study of eight children, aged 3-13 years. b Two hours before the
start of each cancer treatment and every six hours thereafter
for 24 hours, the children were given ![]() 8THC
as oil drops on the tongue or an a bite of bread (18 mg/m2
body surface area). The children received a total of 480 treatments.
The only side effects reported were slight irritability in two
of the youngest children (aged 3.5 and 4 years). Based on the
prediction that the THC-induced anxiety effects would be less
in children than in adults, the authors used doses that were higher
than those recommended for adults (5-10 mg/m2 body
surface area).
8THC
as oil drops on the tongue or an a bite of bread (18 mg/m2
body surface area). The children received a total of 480 treatments.
The only side effects reported were slight irritability in two
of the youngest children (aged 3.5 and 4 years). Based on the
prediction that the THC-induced anxiety effects would be less
in children than in adults, the authors used doses that were higher
than those recommended for adults (5-10 mg/m2 body
surface area).
Antiemetic Properties of Synthetic THC Analogues
Antiemetic Properties of Marijuana
b Note that the authors of this study chose to use
![]() 8-THC
because it is more stable and easier to produce than
8-THC
because it is more stable and easier to produce than ![]() 9-THC;
it does not follow from this particular study that marijuana,
with its mixture of cannabinoids, should be a more powerful antiemetic
than
9-THC;
it does not follow from this particular study that marijuana,
with its mixture of cannabinoids, should be a more powerful antiemetic
than ![]() 9-THC.
9-THC.
Side Effects Associated with THC/Marijuana in Antiemetic Therapy
Therapy for Chemotherapy-Induced Nausea and Vomiting
Present Therapy
antagonist, complete control of acute cisplatin-induced emesis was observed in about 75 percent of patients. In tests where the chemotherapy was only moderately emetogenic, as many as 90 percent of the patients who received these combinations achieved complete control of emesis. Side effects of those antiemetic agents include headache, constipation and alterations in liver function, but are generally well tolerated by most patients. 14
SIDEBAR: Attitudes of Oncologists Toward Prescribing Marijuana
In the 1990s two groups of investigators conducted three surveys on the attitudes of clinical oncologists toward prescribing marijuana as an anti-emetic. These studies are arguably out of date, because the antiemetics that are available now are so much more effective than they were when these studies were conducted. Nonetheless, the studies merit attention because they are still frequently cited as evidence for or against the use of marijuana as an antiemetic. The results of the two groups were contradictory. In 1994, by which time serotonin receptor antagonists (5-HT receptors had become available, Schwartz and Beveridge174 concluded that oncologists had little interest in prescribing marijuana to control emesis, whereas Doblin and Kleiman concluded in 1991 that interest was great.40 Since 1994 the two groups have debated in the literature as to which study represents the true sentiment among oncologist.39, 175, 180 In fact. there are numerous methodological differences between the two studies that might explain the different results.39, 175 Nonetheless, ultimately these studies are irrelevant. Both studies deal with perceptions rather than pharmacological realities based on well-designed outcome studies.180
antiemetic studies with cannabinoids present methodological difficulties and are inconclusive. If one concentrates on the well-conducted trials, the evidence indicates that cannabinoids reduce emesis in about one quarter of patients receiving cancer chemotherapy Cannabinoids are not as effective as several other classes of agents, such as substituted benzamides, serotonin receptor antagonists and corticosteroids. The side effects associated with cannabinoid use are generally tolerable. As with cannabinoids, efficacy was apparent with smoked marijuana, but the degree of efficacy was no better than that seen with available antiemetic agents now considered to be marginally satisfactory. At present, the most effective antiemetic regimens are combinations of oral serotonin receptor antagonists with dexamethasone in single dose regimens given prior to chemotherapy. Neither multiple dose regimens nor intravenous antiemetics provide better control, and both add unnecessary costs. 63, 85
Future Therapy
c Neurokinin receptors are found in brain and the gut and thought to be involved in motor activity, mood, pain, and reinforcement. They may well be involved in mediating gut sensations, including nausea.
Conclusions and Recommendations: Chemotherapy-induced nausea
Wasting Syndrome and Appetite Stimulation
nutrients. Both wasting (cachexia) and anorexia are common end-stage features of certain fatal diseases such as AIDS as well as metastatic cancers. In AIDS, weight loss of as little as 5 percent is associated with decreased survival, and a body weight about one-third below ideal body weight results in death.103, 161
Malnutrition in HIV-Infected Patients
d Body cell mass is the fat-free cellular mass. It is composed of the cells of the muscle and organs, plus circulating hematopoietic cells and the aqueous compartment of adipocytes. It is not fat, extracellular water, or extracellular solids (such as tendons, etc.).
malabsorption; serious systemic infection; focal or diffuse neurological disease; HIV enteropathy, depression; fatigue; and poverty. Nutrient malabsorption is often the result of microorganism overgrowth or infection in the gut, especially in the later stages of AIDS. 99, 159
Marijuana, THC, and in HIV-Infected Patients
e Megestrol acetate is a synthetic derivative of progesterone that can stimulate appetite and cause significant weight gain when given in high doses (320 to 640 mg/d) to AIDS patients.58
Therapy for Wasting Syndrome in HIV-Infected Patients
Present Therapy
Future Therapy
Malnutrition in Cancer Patients
Anorexia Nervosa
dysphoria is that THC increases appetite and thus intensifies the mental conflict between hunger and food refusal.14 malnutrition.199 Furthermore, such patients may have underlying psychiatric disorders (schizophrenia, depression) in which cannabinoids might be hazardous (see chapter 3 Psychological Harms).
Recommendations
Neurological Disorders
Muscle Spasticity
extensor spasms). In some cases these contractions are debilitating and very painful, and require therapy to relieve the spasms and associated pain.
Multiple Sclerosis
f Myelin is the lipid covering that surrounds nerve cell fibers and facilitates the conduction of signals along nerve cells and ultimately between the brain, spinal cord and the rest of the body.
FIGURE 4.2 Effect of nabilone on multiple sclerosis symptoms
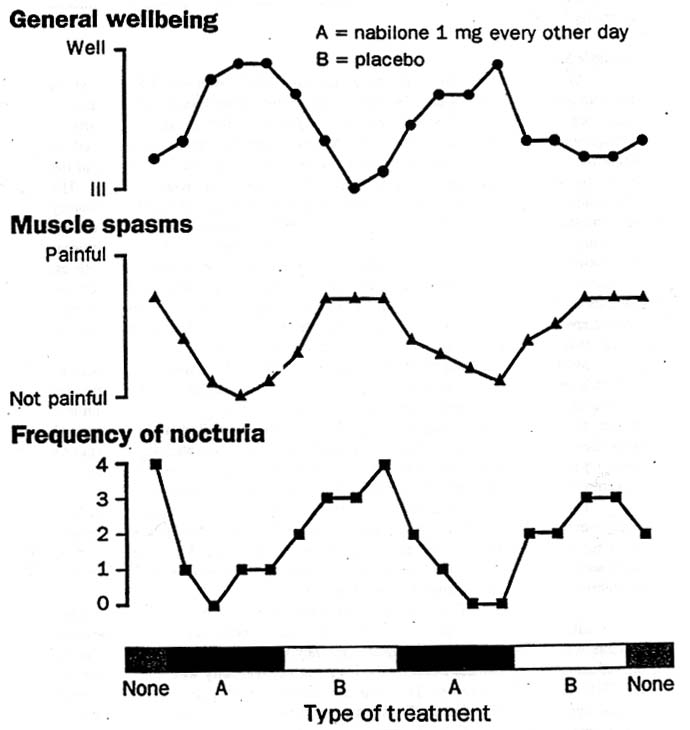
FIGURE LEGEND 4.2
g The pendulum test is an objective and accurate measure of MS-induced spasticity. It is done by videotaping a patient who lies supine on a table with his or her leg extending off the edge. The leg is dropped and the resulting motion is mathematically analyzed by computer to provide a quantitative measure of spasticity.